Designing a low-cost, open source ventilator with Arduino
— March 17th, 2020
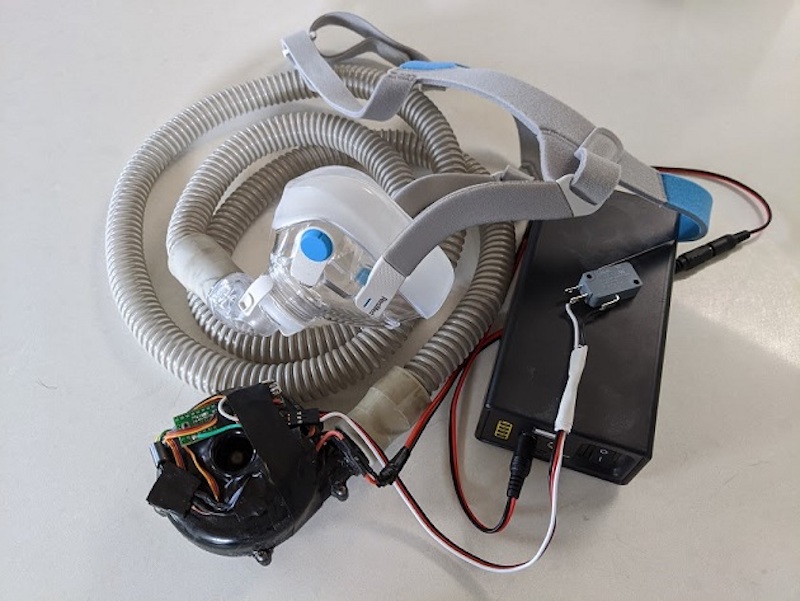
Desperate times call for desperate measures, and while making your own medical equipment isn’t normally advisable, Johnny Lee’e project explores how to turn a CPAP machine into a ventilator.
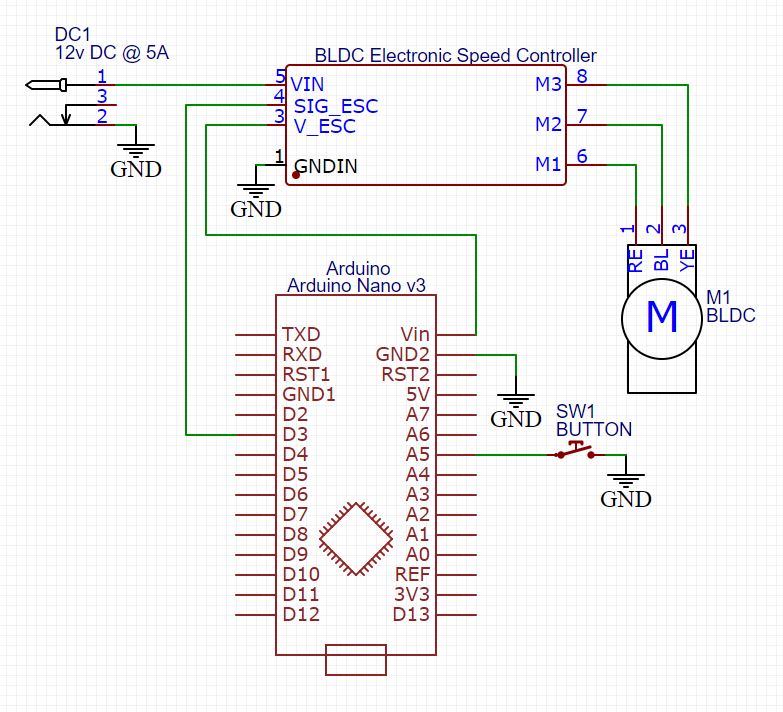
The idea is that since these machines are basically just blowers controlled by a brushless DC motor, an Arduino Nano equipped with an electonic speed controller could allow it to act as a one.
Such a setup has been shown to provide more than enough pressure for a ventilator used on COVID-19 patients. This device has in no way been evaluated or approved for medical use, but it does provide a starting point for experimentation.
You can find additional details, including an air filtration system, on Lee’s GitHub page.
Boards:Nano